Mission: TO PREVENT DANCE INJURIES
Dancing is one of the most physically straining exercises on the body. The types of musculoskeletal injuries, locations, and rates of dance-related injuries are similar to those sustained by traditional athletes. However, dance is more often dismissed as an art form, rather than an athletically demanding sport. The injuries specific to dance vary between the different genres of dance. Therefore, it has been suggested by Roberts, Nelson, and Mckenzie (2013) that prevention strategies need to be focused on preventing injuries in classical dancers, such as in ballet.
Dance-related injuries do not have to be an inevitable fate, especially for young dancers. We are beginning to take steps towards reducing the likelihood and number of dance sustained injuries by focusing on injury screening, strength and conditioning.
The first national study to track dance-related injuries in children and adolescents was published in 2013 by Roberts et al. from The Research Institute at Nationwide Children’s Hospital. These researchers analyzed over 17 years, from 1991-2007. They found that injuries among young dancers have dramatically increased by 37 percent. In 2007 alone, more than 8,000 young dancers were treated in ERs across the U.S. That's nearly an injury per hour, every hour of every day. ”Ballet accounted for 11.7% of all dance-related injuries. Ballet involves repetitive, rotational movements and pointe work which may be physically taxing on the body of a young dancer and lead to injuries” (Roberts et al., 2013, p. 148). The Performing Arts Medicine program was created in response to these research findings. The components identified in this program helped set the foundation for an injury prevention initiative by aiding in the identification of these dancer’s specialized needs and injury risks that are commonly overlooked.
The steps of injury prevention include, increasing injury awareness, dance specific injury screening, implementing a Pilates-based conditioning regimen among our dancers, and additionally evaluating safety measures for pointe work.
Secondly, the study by Galantino, Lim, Bahring, and Woolverton (2017) has inspired the injury screening strategy and main interventions of this project. The dance specific injury screening (DSIS) was created around 3 of the basic steps: plie, releve and saute using observation of the last two movements with double and single leg variations to assess for unilateral differences and deviations from what is considered proper technique. The various fundamental aspects of dance are evaluated by using the four basic movements, plie, releve, saute and temps leve as well as the coupe or cou-de-pied position. A screening will be performed before intervention to assess their risks.
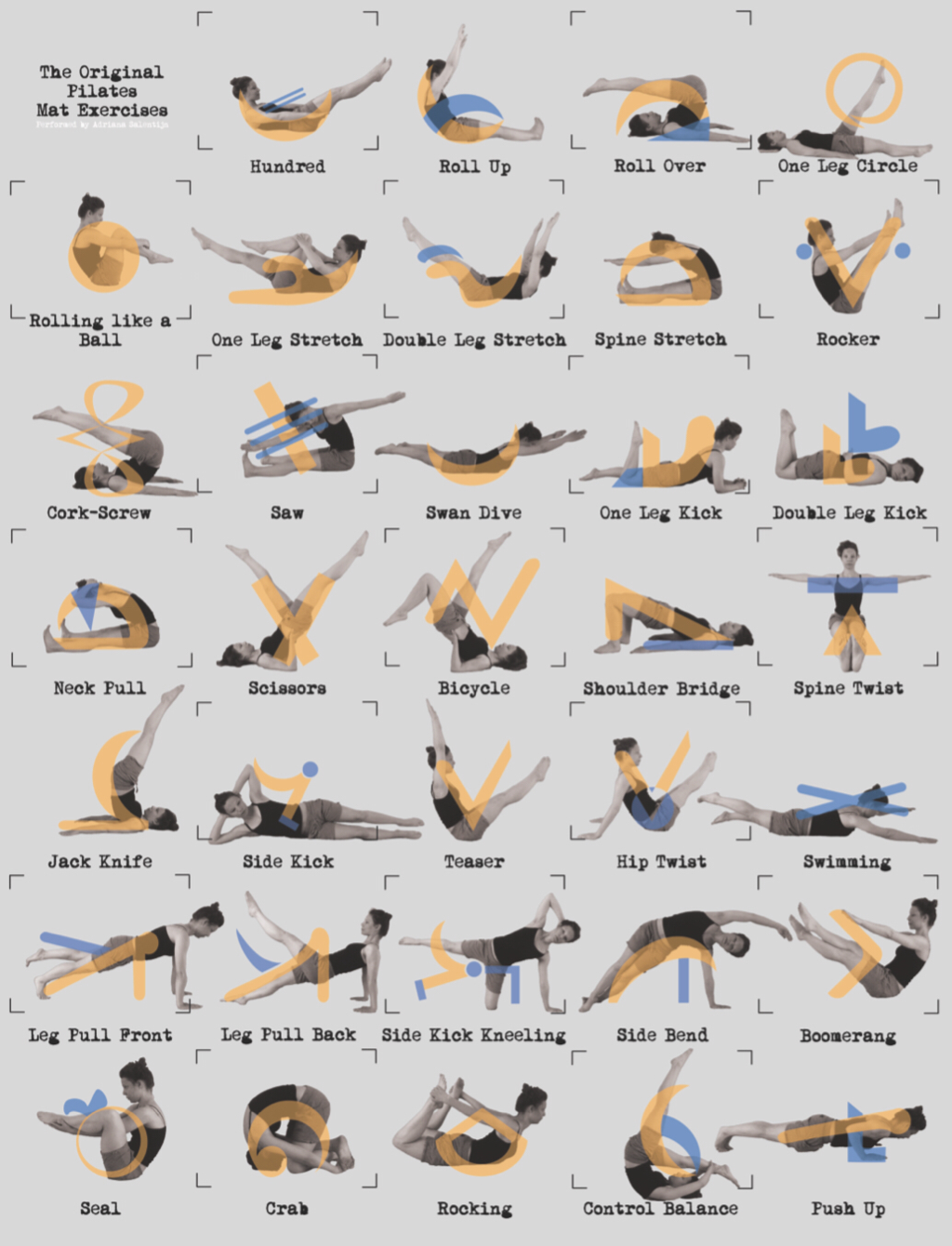
The intervention that will condition these ballet dancers to prevent musculoskeletal injuries will be based on the same Pilates-based approach used in the study by Galantino et al., (2017). These Pilates-based exercises were shown to have a positive influence in improving the group’s DSIS performance score after the six week intervention period. The focus of this conditioning principle is on the core strength and stabilization before working the peripheral parts of the body. Additionally, flexibility is a significant aspect of dance training as greater mobility provides dancers with better full-body integration as well as less chance of joint injury (Galantino et al., 2017). Specifically, lumbo-pelvic flexibility is especially important in performing basic technique exercises. In a study involving healthy adults, there were noticeable improvements in pelvic stability and flexibility in both 4-week and 8-week Pilates training (Phrompaet, Paungmali, Pirunson, & Sitilertpisan, 2011). These exercises will be used as a part of the group warm up before rehearsals and will be led by the instructors of the ballet company. I will be present for the first couple of rehearsal days to ensure the exercises are well understood, and to answer any questions.
Dance-related injuries do not have to be an inevitable fate, especially for young dancers. We are beginning to take steps towards reducing the likelihood and number of dance sustained injuries by focusing on injury screening, strength and conditioning.
The first national study to track dance-related injuries in children and adolescents was published in 2013 by Roberts et al. from The Research Institute at Nationwide Children’s Hospital. These researchers analyzed over 17 years, from 1991-2007. They found that injuries among young dancers have dramatically increased by 37 percent. In 2007 alone, more than 8,000 young dancers were treated in ERs across the U.S. That's nearly an injury per hour, every hour of every day. ”Ballet accounted for 11.7% of all dance-related injuries. Ballet involves repetitive, rotational movements and pointe work which may be physically taxing on the body of a young dancer and lead to injuries” (Roberts et al., 2013, p. 148). The Performing Arts Medicine program was created in response to these research findings. The components identified in this program helped set the foundation for an injury prevention initiative by aiding in the identification of these dancer’s specialized needs and injury risks that are commonly overlooked.
The steps of injury prevention include, increasing injury awareness, dance specific injury screening, implementing a Pilates-based conditioning regimen among our dancers, and additionally evaluating safety measures for pointe work.
Secondly, the study by Galantino, Lim, Bahring, and Woolverton (2017) has inspired the injury screening strategy and main interventions of this project. The dance specific injury screening (DSIS) was created around 3 of the basic steps: plie, releve and saute using observation of the last two movements with double and single leg variations to assess for unilateral differences and deviations from what is considered proper technique. The various fundamental aspects of dance are evaluated by using the four basic movements, plie, releve, saute and temps leve as well as the coupe or cou-de-pied position. A screening will be performed before intervention to assess their risks.
The intervention that will condition these ballet dancers to prevent musculoskeletal injuries will be based on the same Pilates-based approach used in the study by Galantino et al., (2017). These Pilates-based exercises were shown to have a positive influence in improving the group’s DSIS performance score after the six week intervention period. The focus of this conditioning principle is on the core strength and stabilization before working the peripheral parts of the body. Additionally, flexibility is a significant aspect of dance training as greater mobility provides dancers with better full-body integration as well as less chance of joint injury (Galantino et al., 2017). Specifically, lumbo-pelvic flexibility is especially important in performing basic technique exercises. In a study involving healthy adults, there were noticeable improvements in pelvic stability and flexibility in both 4-week and 8-week Pilates training (Phrompaet, Paungmali, Pirunson, & Sitilertpisan, 2011). These exercises will be used as a part of the group warm up before rehearsals and will be led by the instructors of the ballet company. I will be present for the first couple of rehearsal days to ensure the exercises are well understood, and to answer any questions.
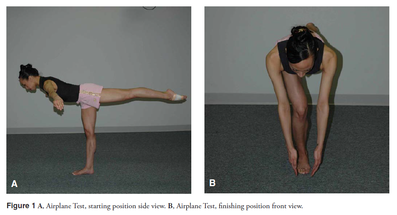
Another aspect of injury prevention will be focused on pointe work safety measures which will include pointe readiness screenings and guidelines for initiating pointe. I will utilize the “Functional Criteria for Assessing Pointe Readiness” by Richardson, Liederback, and Sandow (2015) from Harkness Center for Dance Injuries in NY. This screening method incorporates three tests, the Topple test, Airplane test, and Single-leg Sauté test, which measure trunk control and dynamic lower extremity alignment. These tests assess the dancer’s ability to maintain neutral alignment and center of mass over the base of support while doing complex movements.

Although this one screening test cannot guarantee success or risks, it can aid in determining a dancer’s readiness to participate in pointe training. These tests were found to be significantly predictive of dance teacher classification, and the results will be shared with the instructors to better understand the individual’s pointe readiness (Richardson et al., 2017).
The “Guidelines for Initiating Pointe Training” developed by Weiss, Rist, and Grossman (2009), will be of assistance to safely assess dancers, as these parameters are based on growth, development, and risks associated with starting pointe too early (see picture to left).
The “Guidelines for Initiating Pointe Training” developed by Weiss, Rist, and Grossman (2009), will be of assistance to safely assess dancers, as these parameters are based on growth, development, and risks associated with starting pointe too early (see picture to left).
Overall, it is believed that this initiative will provide solid injury prevention methods that will work to improve flexibility and enhance control-mobility of the trunk and pelvis. As indicated by the study by Galantino et al., (2017), Pilates-based exercises improved the overall group’s DSIS performance score. I predict that this project intervention will have similar results because the majority of these dancers have not received structured conditioning in the past, which could be the underlying cause of the many serious injuries that occur. There are some limitations to the screenings because they are not going to be foolproof determinants for identifying all injuries that have the potential to happen. However, I do believe that the screening tests I have chosen to model my subsequent intervention are reliable and have legitimate reasoning to support their use. I believe incorporating new exercises will be a fairly smooth transition because they resemble the nature of exercises utilized by dancer’s warmups.
Unlike traditional athletes, losing a few degrees of motion in an ankle or hip could potentially be career ending for a ballet dancer. If there is a decline in ability to dance ballet as a result of considerable minor injuries and the dancer is not managed appropriately, there could be detrimental injuries. With all these aspects considered, I hope to make a difference within this dance community of Oak Ridge and work towards promoting a culture of safety and wellness.
References:
Galantino, M. L., Lim, J. H., Bahring, S., & Woolverton, K. (2017). Outcome measures for
dance injury: A pilot study exploring functional movement screen and a novel screening
tool. Orthopaedic Physical Therapy Practice, 29(3), 168-173.
Phrompaet, S., Paungmali, A., Pirunson, U., & Sitilertpisan, P. (2011). Effects of pilates training
on lumbo-pelvic stability and flexibility. Asian J Sports Med; 2(1): 16-22.
Richardson, M., Liederbach, M., & Sandow, E. (2015). Functional criteria for assessing pointe
readiness. International Association for Dance Medicine & Science, 6(1), 6-7.
Roberts, K. J., Nelson, N. G., & Mckenzie, L. (2013). Dance-related injuries in children and
adolescents treated in US emergency departments in 1991−2007. Journal of Physical
Activity and Health, 10(2), 143-150. doi:10.1123/jpah.10.2.143
Weiss, D. S., Rist, R. A., & Grossman, G. (2009). When can I start pointe work? Guidelines for
initiating pointe training. International Association for Dance Medicine & Science,
13(3), 90-92.
Unlike traditional athletes, losing a few degrees of motion in an ankle or hip could potentially be career ending for a ballet dancer. If there is a decline in ability to dance ballet as a result of considerable minor injuries and the dancer is not managed appropriately, there could be detrimental injuries. With all these aspects considered, I hope to make a difference within this dance community of Oak Ridge and work towards promoting a culture of safety and wellness.
References:
Galantino, M. L., Lim, J. H., Bahring, S., & Woolverton, K. (2017). Outcome measures for
dance injury: A pilot study exploring functional movement screen and a novel screening
tool. Orthopaedic Physical Therapy Practice, 29(3), 168-173.
Phrompaet, S., Paungmali, A., Pirunson, U., & Sitilertpisan, P. (2011). Effects of pilates training
on lumbo-pelvic stability and flexibility. Asian J Sports Med; 2(1): 16-22.
Richardson, M., Liederbach, M., & Sandow, E. (2015). Functional criteria for assessing pointe
readiness. International Association for Dance Medicine & Science, 6(1), 6-7.
Roberts, K. J., Nelson, N. G., & Mckenzie, L. (2013). Dance-related injuries in children and
adolescents treated in US emergency departments in 1991−2007. Journal of Physical
Activity and Health, 10(2), 143-150. doi:10.1123/jpah.10.2.143
Weiss, D. S., Rist, R. A., & Grossman, G. (2009). When can I start pointe work? Guidelines for
initiating pointe training. International Association for Dance Medicine & Science,
13(3), 90-92.